Chest wall schwannoma – CXR, CT and MRI
This woman, in her mid-30s, presented to the ED with dyspnoea and had a chest radiograph as part of her work-up.
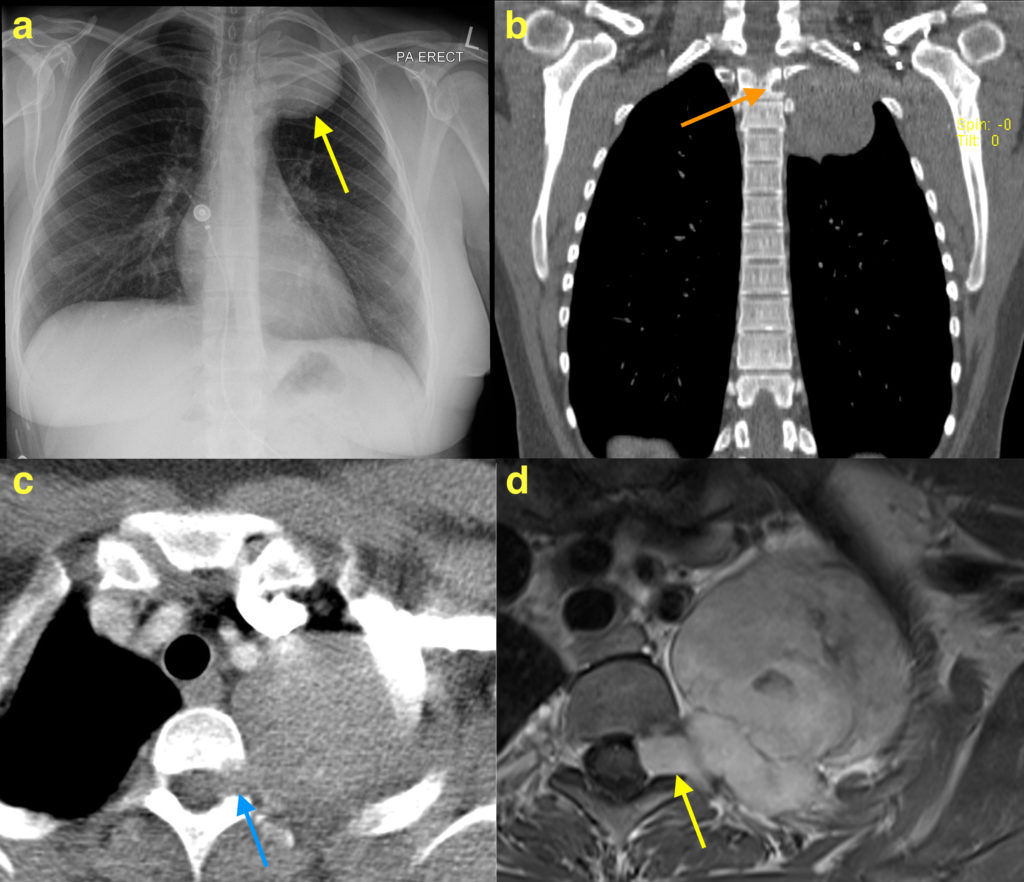
This showed a large rounded mass at the left apex (arrow on image (a)). Although not responsible for her dyspnoea, this incidental finding required further imaging for characterisation so both CT and MRI were performed.
On the CXR, the mass was considered likely to be either pleural-based or extra-pleural (i.e. arising from components of the chest wall) rather than the lung itself. However, it can be difficult to be certain of this on radiographs – helpful signs include the fact that only a portion of the margin of the mass is outlined by aerated lung. Extra-pleural masses frequently erode the adjacent rib(s), which another helpful feature.
The differential diagnosis for a pleural or extra-pleural mass is quite wide, and includes the following:
Pleural masses:
Benign lesions
Pleural thickening
Loculated pleural effusion
Empyema
Haematoma
Lipoma
Fibroma
Malignant lesions
Metastases (e.g. lung, breast ca)
Mesothelioma
Lymphoma
Extra-pleural masses:
Benign lesions
Tumours of peripheral nerves (neurofibroma, schwannoma)
Rib lesions (e.g. osteochondroma, fibrous dysplasia)
Haematoma (e.g. due to rib fracture)
Malignant lesions
Rib myeloma/plasmacytoma
Rib metastases
Chondrosarcoma
Ewing sarcoma (a.k.a. primitive neuroectodermal tumour or Askin tumour)
Although the differential diagnosis is long, there is a very helpful clue in this example – the mass has eroded the adjacent vertebra (arrow on CT image (b)) and has extended into the neural exit foramen (arrows on CT image (c) and post-contrast T1-weighted MRI image (d)). This is a very typical feature of nerve sheath tumours, most commonly neurofibromas or schwannomas, and rarely occurs with the other lesions listed above.
Biopsy of this lesion was performed under ultrasound-guidance and confirmed that it was a schwannoma.
In the chest wall, schwannomas can arise from either the spinal nerve roots or the intercostal nerves and are usually encountered in young to middle-aged adults. On CT, schwannomas are usually of similar density to muscle (as in this example). On MRI, they are usually of slightly higher (brighter) signal to muscle on T1-weighted imaging, of much higher signal than muscle on T2-weighted imaging, and show avid enhancement when intravenous gadolinium contrast is given.