Small bowel obstruction due to port site hernia – CT
One of the great advantages of CT over radiography in the patient with small bowel obstruction is that is often allows us to tell the surgeon the exact cause.
In this example, a young female patient presented to the ED one month after undergoing a diagnostic laparoscopy, complaining of nausea, vomiting, abdominal pain and distension. A plain film showed dilated (i.e. > 3 cm) small bowel loops indicating obstruction, and a CT was requested.
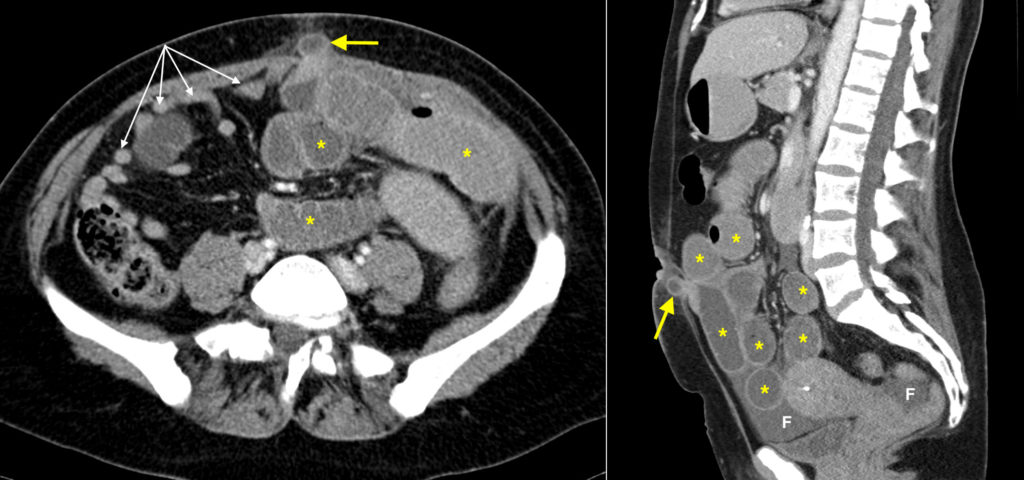
On the transverse (left) and sagittal CT images shown here, multiple dilated small bowel loops are shown (marked with ‘*’). There is also some free fluid (F) in the pelvis, which is often seen in the setting of bowel obstruction. One of the important things we look for on a CT in bowel obstruction is what is known as the ‘zone of transition’, which is the exact point at which the dilated bowel changes to being non-dilated and indicates the site of the obstructing lesion. Beyond this point, the bowel is often completely collapsed (as in this example – the collapsed ileal loops are indicated by the white arrows).
In this case, the cause of the obstruction was herniation of small bowel through the recent umbilical incision that had been used for the laparoscopy port (a knuckle of bowel is protruding through the defect in the abdominal wall, yellow arrow). The patient was brought to theatre to have the hernia reduced and the defect closed.
CT is widely used in the work-up of patients with small bowel obstruction and its role is to answer several specific questions:
- Is the bowel definitely obstructed?
- If so, is it only small bowel or is the colon dilated also?
- Where is the zone of transition from dilated to non-dilated bowel?
- Is a cause for the obstruction visible?
- Are there any associated complications (e.g. ischaemia, perforation)?