Typhlitis
This 50-year-old man had a history of acute lymphocytic leukaemia (ALL) and was undergoing chemotherapy for this. During treatment, he presented with acute onset of right lower quadrant pain and fever.
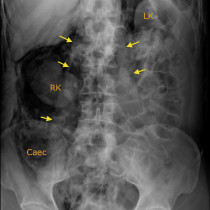
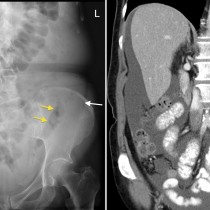
This CT shows typical features of a condition called ‘typhlitis’, also known as neutropenic colitis. This classically involves the caecum, often extending to involve the ascending colon, appendix and, in some cases, the terminal ileum.
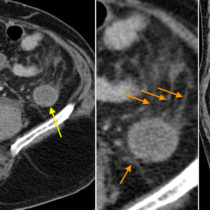
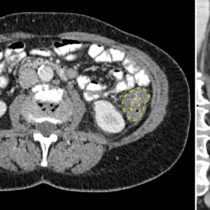
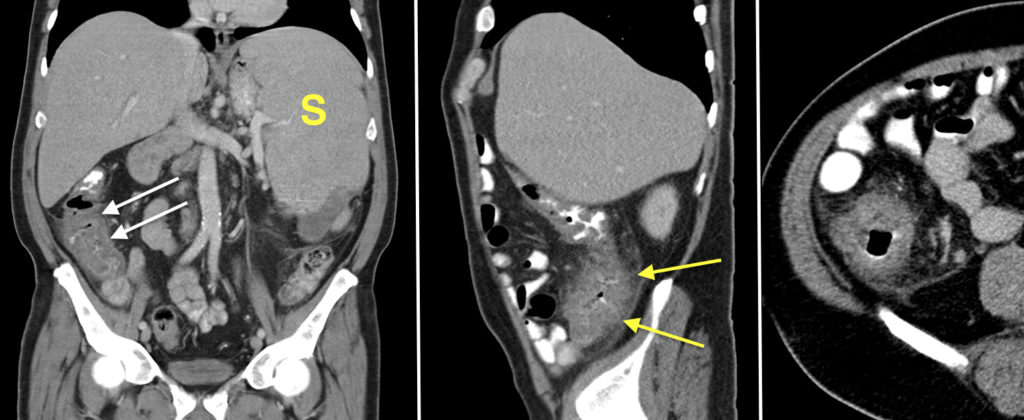
The coronal CT image on the left shows thickening and oedema of the wall of the ascending colon, arrows. Note the enlarged spleen ‘S’, related to his underlying diagnosis of ALL. On the middle, sagittal image, you can see haziness (‘stranding’) of the fat adjacent to the caecum and ascending colon (arrows). The transverse image on the right also shows the circumferential thickening of the caecal wall.
Typhlitis is seen in immunocompromised patients, particularly those with an underlying haematological malignancy. The aetiology is considered to be multifactorial, involving a combination of relative ischaemia, the immunocompromised status of the patient, infection with various organisms (e.g. CMV, E. coli, C. difficile), and possibly mucosal infiltration by the underlying malignancy.
Management is with intensive antimicrobial treatment. Surgery is occasionally required when the process is complicated by pneumatosis or frank perforation. Mortality is reported to be up to 50%.
The differential diagnosis for this appearance would include right-sided diverticulitis, appendicitis (although the extent of the colonic wall thickening usually helps differentiate this), and inflammatory bowel disease. The clinical history is, of course, very helpful in making the correct diagnosis.